Gallbladder Diseases
Functions of Gallbladder
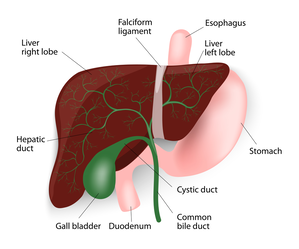
The gall bladder is a small pear-shaped organ attached to the side of the bile duct by a small secondary duct, the cystic duct. The bile duct is a tube that carries bile from the liver to the small intestine. When the patient is fasting, the lower end of the bile duct closes and bile back-flows into the gall bladder. There it is concentrated by the gall bladder, absorbing the water in the bile. When a patient eats a fatty meal, the gall bladder squeezes out the bile to help absorb the fats. If stones are present, they can cause the gall bladder to go into spasm and causes severe pain as well as nausea, vomiting, bloating, or fever. If a gallstone travels down the bile duct, you could have liver dysfunction, bile duct infection or inflammation in the pancreas, called pancreatitis. The only way to prevent this and the other problems that can occur with gall stones is to remove the gall bladder. Since the gall bladder is only one of the mechanisms of fat digestion, its removal does not cause any major interference with the patient’s digestive process. In many cases of patients with stones, the gallbladder is not functioning and so digestion of fats is not affected by its removal.
Gallstones
If the bile contains too much cholesterol or bilirubin, or the gallbladder does not empty properly, then stones can form within the gallbladder. Gallstones can be cholesterol stones, pigment stones or a mixture of the two. Cholesterol stones are largely made of solidified cholesterol. Pigment stones are dark stones made of bilirubin. The majority of stones are mixed stones that contain cholesterol as well as pigment. The gallbladder can develop just one or two large stones (some can be as large as a golf ball), or lots of tiny stones (as small as grains of sand).
Causes of Gallstones
The gallbladder is a small organ in the right upper abdomen under the liver. When healthy, it stores some of the bile that is made by the liver. Bile is necessary to digest and absorb the fats in the foods we eat. When there is an imbalance of the chemicals in the bile, gallstones can form.
A number of causes have been suggested. It is thought that some people secrete more cholesterol than others. As the gallbladder concentrates the bile stored in it, the cholesterol precipitates forming crystals and these adhere together forming the stones. The stones then tend to enlarge or multiply especially if there is any infection involved. Pregnancy, obesity, weight loss and a family history of gallstones are factors that increase the chances of developing gallstones.
Risk Factors for Gallstones
Women, particularly between the ages of 20 and 60 years, are more likely to form gallstones than men. In general, those over 60 (men and women) are at a higher risk of developing gallstones. People who are overweight are more likely to form gallstones. Excess estrogen from numerous pregnancies, hormone replacement therapy, or birth control pills may increase cholesterol levels in bile, slow down gallbladder emptying, and lead to gallstones.
People who have biliary infections (for example liver flukes in the tropics) can develop gallstones. Individuals with hereditary blood disorders such as sickle cell anemia (in which too much bilirubin is formed due to the breakdown of blood cells) are more likely to form pigment stones. Going on a diet (with rapid weight loss) and certain cholesterol-reducing drugs can also increase the risk of gallstone formation. A high level of cholesterol in the blood is not necessarily a factor in the development of gallstones. Many people have a “family history” of gallstones but there is no particular gene that has been associated with this.
Prevention of Gallstones
There is no special diet you can follow, particular foods you should avoid, or medications you can take to specifically prevent the formation of gallstones. Those who already have pain from gallstones often find that fatty or oily food can trigger the pain. So a low-fat diet can help keep the pain at bay. Gallstones are not related to stones in other parts of the body, particularly stones in the kidneys or in the urinary bladder.
Symptoms of Gallstones
The main symptom is pain, known as gallstone or biliary colic. This commonly occurs in the mid upper abdomen or under the right ribs. It tends to radiate around the rib margin and into the back. It can be precipitated by eating fats. It is severe and can last some hours. The pain usually goes but frequently recurs. In some cases infection sets in, cholecystitis, and the patient develops severe pain under the right ribs with fever. Intravenous antibiotics are necessary to treat the infection and the problem usually takes 3-4 days to settle. If a gallstone passes down the cystic duct into the bile duct it can block the flow of bile leading to jaundice. This is a surgical emergency requiring removal of the obstruction, especially if infection sets in. A stone in the bile duct may also cause inflammation of the pancreas causing a serious condition known as pancreatitis. Rarely, if the stones are left for many years, cancer of the gall bladder may develop.
Often, gallstones remain “silent” and do not cause any symptoms at all. Silent gallstones are usually discovered by accident when tests are done for other problems. The milder symptoms of gallstones include abdominal bloating, belching, indigestion, and nausea, usually after a meal. More severe symptoms include attacks of abdominal pain and vomiting. The pain is usually in the upper abdomen, often more to the right, and can move to the right shoulder blade or shoulder tip. It may come on after meals, especially with fatty foods. This kind of pain is called biliary colic. Most attacks of biliary colic settle after a few hours.
Gallstone can cause symptoms similar to those of a heart attack, appendicitis, bowel obstruction, peptic ulcer, hiatus hernia, pancreatitis, hepatitis and occasionally biliary cancer. It is therefore very important that the correct diagnosis is made.
Diagnosis of Gallstones
To determine if you have gallstones, you will likely undergo an ultrasound, which uses sound waves to detect gallstones and evaluate the bile ducts. If there are abnormalities in the pancreas or bile ducts, additional imaging tests including a CAT scan or magnetic resonance cholangiopancreatography (MRCP), may be necessary. Blood tests can also be helpful if infection or bile duct blockage is suspected.
Complications Caused by Gallstones
Gallstones can lead to acute inflammation of the gallbladder (cholecystitis). Acute cholecystitis is a medical emergency and requires admission to hospital. Treatment has conventionally involved pain killers and antibiotics to settle the acute inflammation, followed six weeks later by an operation to remove the gall bladder. Current best practice involves operating immediately with laparoscopic surgery and this has lead to better outcomes.
Acute cholecystitis caused by aggressive bacteria can cause the gall bladder wall to rot and disintegrate, and the gall bladder may then burst into the abdominal cavity or into an adjacent bit of bowel.
If there have been repeated attacks of inflammation, the gall bladder becomes chronically inflamed, shrunken and scarred. This is called chronic cholecystitis. If the outflow from the gall bladder is totally blocked by a stone it may become a bag full of stagnant bile (a mucocoele) or a bag of pus (empyema).
Gallstones slipping out of the gallbladder into the bile duct can block the flow of bile and cause obstructive jaundice. If you have severe abdominal pain, chills, fever, yellow discoloration of the eyes or skin, or pale stools, you should urgently consult a doctor.
Gallstones passing down the bile duct may also cause inflammation of the pancreas, Acute pancreatitis is a medical emergency, which occasionally escalate into life-threatening complications.
Gallstones Vs. Gallbladder Cancer
Although gallstones are a common problem, gallbladder cancer is a rare form of cancer except in certain parts of the world and in some ethnic groups. Underlying genetic or dietary factors may be the reason for this.
Gallstones are a risk factor for gallbladder cancer, though the mechanism is unclear. Usually patients with large stones of long duration are at increased risk for cancer. More than the stones themselves, incomplete emptying of the gall bladder and the chronic inflammation that goes with it may have a role to play in initiating the cancer. Calcium deposits in the wall of the gallbladder (a consequence of chronic inflammation), described as Porcelain gall bladder, increase the risk of gall bladder cancer. The picture on this page shows a CT scan, with a porcelain gall bladder clearly visible (you can click on the picture to enlarge it). Chronic Salmonella infection of the gall bladder, which predisposes to gallstone formation, can predispose to gallbladder cancer.
Patients with choledochal cysts (a focal or diffuse bulge in the bile duct) or abnormalities at the point where the pancreatic and bile ducts join and enter the bowel are also known to be at increased risk for gallbladder or bile duct cancer. Sometimes patients are found to have polyps (little growths) on the lining of the gallbladder. Polyps are generally benign, but patients with a single, large (> 1cm) polyp are more likely to develop cancer within their polyp. See below for more information about gall bladder polyps.
Gallbladder Polyps
Polyps are growths on the inner lining of the gall bladder wall. Gallbladder polyps are often discovered incidentally on scans, and not all of them warrant removal. Polyps that are single, sessile (do not have a stalk), and are 1 cm or more in diameter should be deemed as suspicious i.e. they may develop into cancerous (malignant) growths. Also, polyps that have developed in older patients (over the age of fifty years), developed in association with stones or are associated with symptoms, are at a higher risk of being malignant or subsequently turning malignant. Laparoscopic cholecystectomy (keyhole surgery to remove the gall bladder) is the treatment of choice in these patients, unless the suspicion of malignancy is high, in which case open exploration is preferable, with preparation for extended resection if necessary.
For polyps that are deemed low-risk, Mr Karametos's practice is to recommend follow-up at first with regular ultrasound scans every 6-12 months, which can stop after 2 years if they remain unchanged.
Other Problems With Similar Symptoms
The symptoms of gallstones can be similar to those of heart disease, appendicitis, bowel obstruction, peptic ulcer, hiatus hernia, pancreatitis, hepatitis and occasionally biliary cancer. It is therefore very important that the correct diagnosis is made. Other tests may be required, including an Gastroscopy to look inside the oesophagus and the stomach.
Treatment for Gallstones

Treatment for Gallstones
Gallstones are best treated by an operation that removes the gallbladder. This is called a cholecystectomy. The traditional method of cholecystectomy was by open surgery through a long cut under the right edge of the rib cage. Today, most cholecystectomies can be performed by the laparoscopic method (also called ‘key hole’ surgery). If the gallbladder is causing symptoms or if multiple small stones that can escape into the bile duct are present, then removal of the gallbladder is advised. The surgery, when performed, entails removal of the whole gallbladder with the stones inside.
To remove only the stones could result in them reforming after several years and problems returning. The gallbladder is not a vital organ, and absorption and digestion can continue normally after it is taken out. If you have gallstones and don’t remove your gallbladder, you risk infection of the gallbladder (cholecystitis) or bile duct obstruction leading to pancreatitis.
Silent Gallstones
Silent gallstones that have been detected by chance and have never caused any symptoms do not need treatment. There may be some unusual circumstances where treatment may be recommended for silent gallstones, such as a strong suspicion of cancer, or a patient who will not cope very well with gall bladder inflammation if it develops – Mr Karametos can discuss these with you However, once gallstones have started to cause symptoms it is likely that they will continue to do so.
Non-Surgical Treatment for Gallstones
Some medicines do exist that may gradually dissolve gallstones, if taken over a period of time. But they only work for a small number of patients, and once the treatment is stopped the stones generally form again. The drugs (ursodeoxycholic acid and chenodeoxycholic acid) work only for small cholesterol stones, and only if the gallbladder empties properly. Months or even years of treatment may be necessary before all the stones dissolve. The drugs may cause mild diarrhea, and one of them may temporarily raise levels of blood cholesterol and certain liver enzymes. These drugs should be offered only to patients who are unfit to undergo surgery. Stones usually recur after these treatments.
Lithotripsy (using sound waves to break up the stones) can work well for kidney stones, but does not work for gallstones. After they have been broken up, the gallstones may not flush out of the gallbladder. In fact the debris can clog the bile duct and cause additional problems.
Endoscopy (ERCP) can get rid of stones in the bile duct, but stones in the gall bladder cannot be removed this way.
Leaving the gallbladder behind and doing an operation to only remove the stones will mean that the stones can form again. So an operation to surgically remove the gallbladder is the best treatment for gallbladder stones that are causing symptoms.
You may have heard of remedies to “flush out” gallstones. These treatments are unproven, and have no solid scientific evidence to support their use. It is possible that these remedies have benefited some individuals, but to be labelled effective, a treatment has to be shown to work in a majority of patients, when compared against another “standard” treatment or against a placebo.
Gallbladder Removal Surgery
Laparoscopic Gallbladder Removal Surgery (Cholecystectomy)
Laparoscopic or keyhole removal of the gall bladder was one of the first procedures to utilise the laparoscopic surgical technique. The procedure has been in use since 1993 in Australia, with many thousands of the procedures being performed. The benefits of the laparoscopic technique include less pain, shorter hospital stays, faster recovery times, fewer post operative small bowel obstructions, and fewer wound infections.
Mr Steven Karametos's standard of care for gallstone disease is laparoscopic cholecystectomy, which is a minimally invasive surgical option for removing the gallbladder. This is a very safe operation.
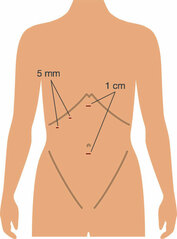
The laparoscopic removal of the gall bladder (cholecystectomy) is performed under general anaesthetic so the patient must be in reasonable health. Mr Karametos makes three or four cuts in the abdominal wall, each of these cuts is generally no more than 1 cm in length. The first is in the umbilicus. The abdomen is then blown up with carbon dioxide (CO2) gas. This lifts the abdominal wall upwards, and gives the surgeon space to operate. After that, telescope attached to a tiny video camera is introduced and the abdominal contents inspected. The gall bladder is readily located and is grasped with forceps. It is freed from attachments to the liver. A small tube, the cystic duct, connecting the gall bladder to the bile duct is dissected free of the fatty tissue that encases it and a catheter inserted into it. Dye is injected down this and an x-ray of the main bile duct, which takes bile from the liver to the intestine, is taken. This is to confirm that no gallstones have entered the bile duct where they could cause a blockage leading to obstructive jaundice. Once the Xray has been completed, the cystic duct and the little artery feeding the gall bladder are clipped with little metal clips and divided. The gallbladder is then dissected away from the liver and removed through the small incision beneath the umbilicus. It is like a small bag that passes through the little incision once the stones and bile have been emptied out of it. The operation usually takes 30 to 90 minutes. At the end of the operation the carbon dioxide gas is let out. Laparoscopic cholecystectomy is preferable to open surgery because the cuts made are much smaller, postoperative pain is less, hospital stay is shorter, and the return to normal activity much quicker.
Open Gallbladder Surgery
In a small number of patients (less than 1 percent), it may not be possible to remove the gallbladder by the keyhole method because of inflammation and scarring around the gallbladder, or the anatomy of the structures is not clear. The risk of conversion to open surgery is higher if you have undergone previous operations on your abdomen or suffered from peritonitis. Other reasons for open surgery include a history of bleeding disorders and with pregnancy.
If laparoscopic cholecystectomy is not possible, Mr Karametos may consider converting the operation to an open surgical operation through a traditional surgical incision. What is done inside is exactly the same, but there is a bigger wound, and therefore a longer convalescence, usually 3-5 days.
Mr Steven Karametos also offers minimally invasive laparoscopic surgical options for common bile duct exploration or stone extraction.
Before Gallbladder Removal Surgery
Diet for Gallstone Patients
If certain fatty foods have triggered your attacks of pain, you should avoid those. In general, you will be better off if you adopt a low fat diet. This will not get rid of your gallstones, but may reduce the severity and frequency of your attacks of pain. Here are some tips:
- Eat less
- Eat only when hungry; stop eating when you are full
- Eat mainly plants; less meat
- Eat fish or poultry in preference to red meat, as red meat contains more fat
- Avoid dairy and egg
- Eat home cooked food (where you can control what goes in, rather than purchased or processed foods)
- Trim all fat and skin off meat when cooking
- When cooking vegetables or meat, try to boil, steam, grill, bake or shallow-fry in a non-stick pan rather than deep-fry or cook in a rich sauce
- When baking cakes, half of the butter can usually be replaced by zero fat yogurt
- When buying food, look at the fat content and opt for low fat version
- Cut down on oily foods, such as deep-fried food, cheesy dishes
For An Attack of Biliary Pain
For a mild attack, try Paracetamol or Ibuprofen (assuming you have no allergies to either of these drugs and no asthma) as well as some anti-acid medication (for example Gaviscon or Omeprazole). Buscopan may help too. If the pain is very severe to start with or does not settle with these medications, please seek urgent medical help. Please remember - just because you have gallstones does not mean you cannot have other problems like angina or acid reflux.
Inflamed Gallbladder & Gallbladder Surgery
Mr Karametos will discuss this with you during consultation. If your attack of acute cholecystitis has started only in the last 7 days, and the diagnosis has been made promptly, then it may be reasonable to proceed immediately to an operation. But with each passing day, the tissues around the gall bladder can become more inflamed and “sticky”, and it may then be safer to wait for 4-6 weeks and let the inflammation settle before doing the cholecystectomy.
Gallbladder Surgery during Pregnancy
Here are a few general guidelines about surgery during pregnancy (other than obstetric operations):
- Elective (non-urgent) operations that can be safely postponed, should be postponed until after delivery.
- If possible, non-urgent surgery should be performed in the second trimester (i.e. months 4,5 and 6).
- A pregnant woman should never be denied emergency surgery for life-threatening conditions, regardless of where she is in the course of her pregnancy.
Pre-Operative Instructions
Prior to your gallbladder surgery, Mr Karametos will spend time with you to explain the procedure and complete Surgery Consent Form during consultation. Our office staff will then provider you with the general Pre/ Post- Operative Instructions to take home. Please do read this document carefully before the surgery, you may also download a copy HERE. Please feel free to call us within business hours on (03) 9857 3600 should you have any other questions.
Hospital Admission Forms
You can complete the hard copy which our staff provides and submit to hospital via mail or in person, Alternatively, you may complete this online. eAdmission forms need to be completed at least 24 hours prior to the procedure. Please follow the links below to complete your admissions form:
Knox Hospital eAdmissions:
http://www.knoxprivatehospital.com.au/index.php/patients/eadmissions-registratio
Mitcham Hospital Online Admissions:
http://www.mitchamprivate.com.au/For-Patients/Online-Admission-Form
Recovery After Gallbladder Removal Surgery
In Hospital
You will wake up feeling drowsy in the operating theatre’s recovery area. You will then be taken back to the ward. There will be some pain and sickness for 12 to 24 hours, but you will be given medications for this. Some bruising and slight oozing of blood around the cuts is normal. Once you are fully awake, you will be encouraged to walk around and drink fluids. You should then be able to eat something light a few hours later.
Wound Care
You will be given pain killers. Please take them as prescribed. Ask Mr Karametos about the care of your wounds. In most instances your cuts will be closed with glue or with self-dissolving stitches under the skin. Waterproof dressings allow for short showers after the surgery. Some pain and mild bruising around the wounds is normal.
Recovery Timeline After Gallbladder Surgery
Usually patients can go home the same or next day post-operatively. One week off work is sufficient for sedentary workers. For those who do heavy lifting, Mr Karametos advises three weeks off to allow the umbilical wound to settle and strengthen. If you want to go to the gym, wait for 2 weeks, and then re-start gently. You will need 5 days before returning to driving. When recovering from a gallbladder operation, If doing something hurts your tummy, then stop doing it.
Postoperative Diet
Surprisingly, removal of the gallbladder seems to have no effect on the digestive process in the vast majority of patients who undergo this operation. The bile trickles steadily into the gut and helps digest the fatty foods. The digestive system just adapts to the absence of the gallbladder. You should be able to continue eating normally after the operation. You do not need to modify your diet because your gallbladder has been removed.
Diarrhoea After Gallbladder Surgery
A small number of people develop frequent loose, watery stools after surgery to remove their gallbladders. In most cases, the diarrhoea resolves soon afterwards. Rarely, it may last longer. The cause of diarrhoea after gallbladder removal is not known. It may be due to more bile acids entering the intestine and acting as a laxative. Please contact Mr Karametos's rooms and we may advises you to try anti-diarrhoeal medications and cut down on foods that can worsen diarrhoea in general, including dairy products, very greasy or sweet foods, and caffeine.
Complications
Every operation inevitably carries a small element of risk, but your surgeon, anaesthetist and nurses will take great care to prevent complications. The likelihood of complications after an operation to remove the gall bladder is very low. There some risks associated with the general anaesthetic, including pneumonia, heart problems, and blood clots in the leg veins and lungs.
If you find any redness or discharge in the wound, get an unusual amount of pain, develop a fever, or develop jaundice (your eyes and skin look yellow), do contact Mr Karametos's rooms or the hospital, as these may be signs of a wound infection or other complications.
Post-Cholecystectomy Syndrome
Around 95% of patients are well and free of symptoms after a cholecystectomy. In a small number of patients the old symptoms may persist, or new symptoms may develop. The term post-cholecystectomy syndrome is sometimes used to describe this situation. The first thing to consider is were the initial symptoms caused not by the gallstones but by some other problem that was not picked up (such as acid reflux or a peptic ulcer or chronic pancreatitis)? Further tests may be required to diagnose these, for example an endoscopy. The second possibility is that there may be a gallstone that has been left behind, perhaps in the bile duct. Blood tests and an ultrasound or MRCP scan can clarify this, and an endoscopic procedure (ERCP) can usually be done to remove the stone.
These are rare problems, but if and when they do occur, you need to have a detailed discussion with Mr Karametos. A careful history and examination, and the correct tests, can often help find the underlying cause, which can then be treated.
Read More About...



